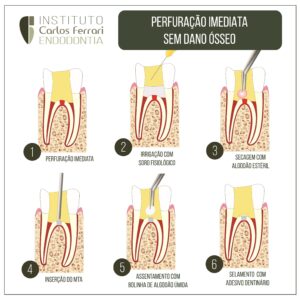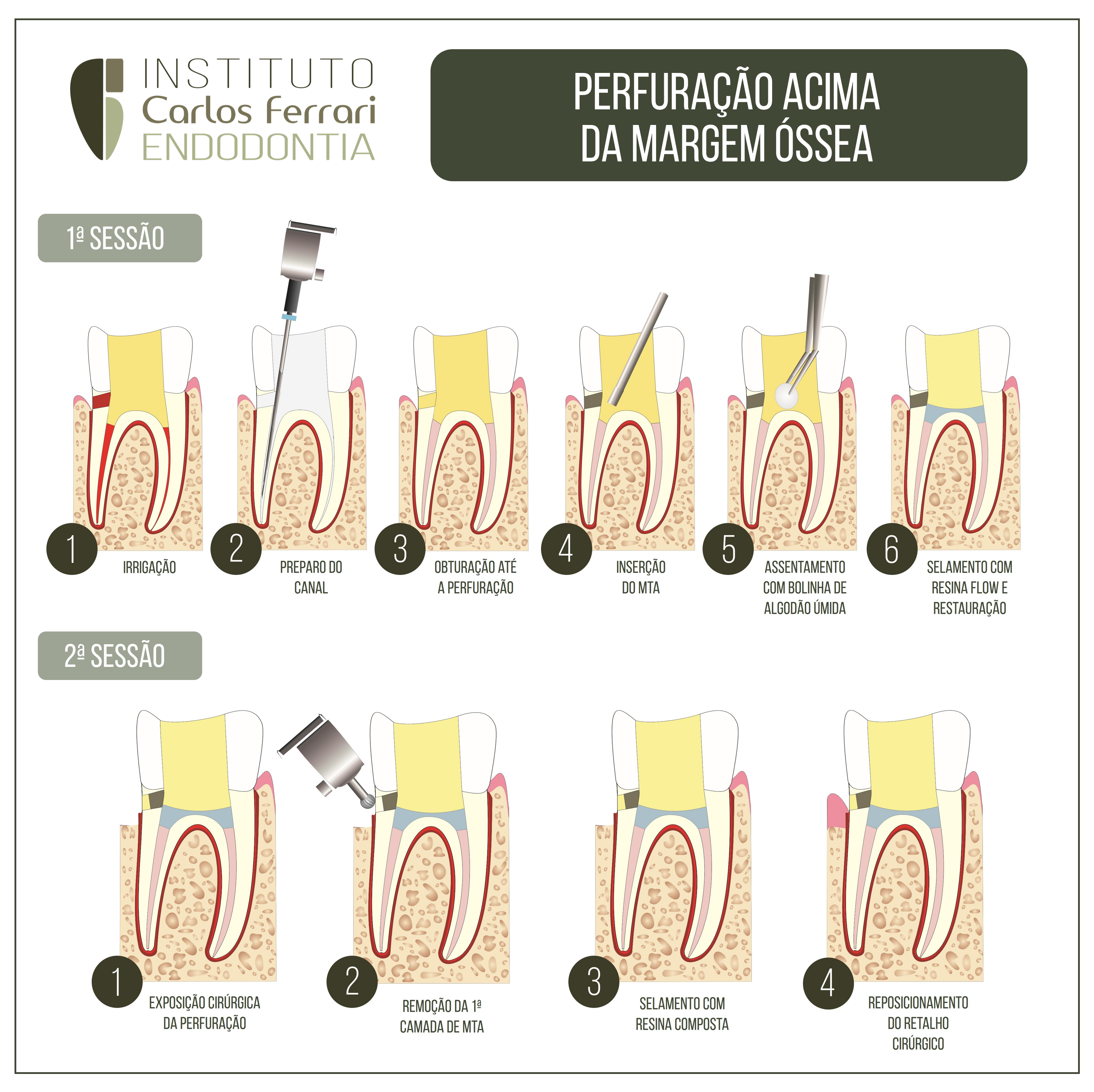
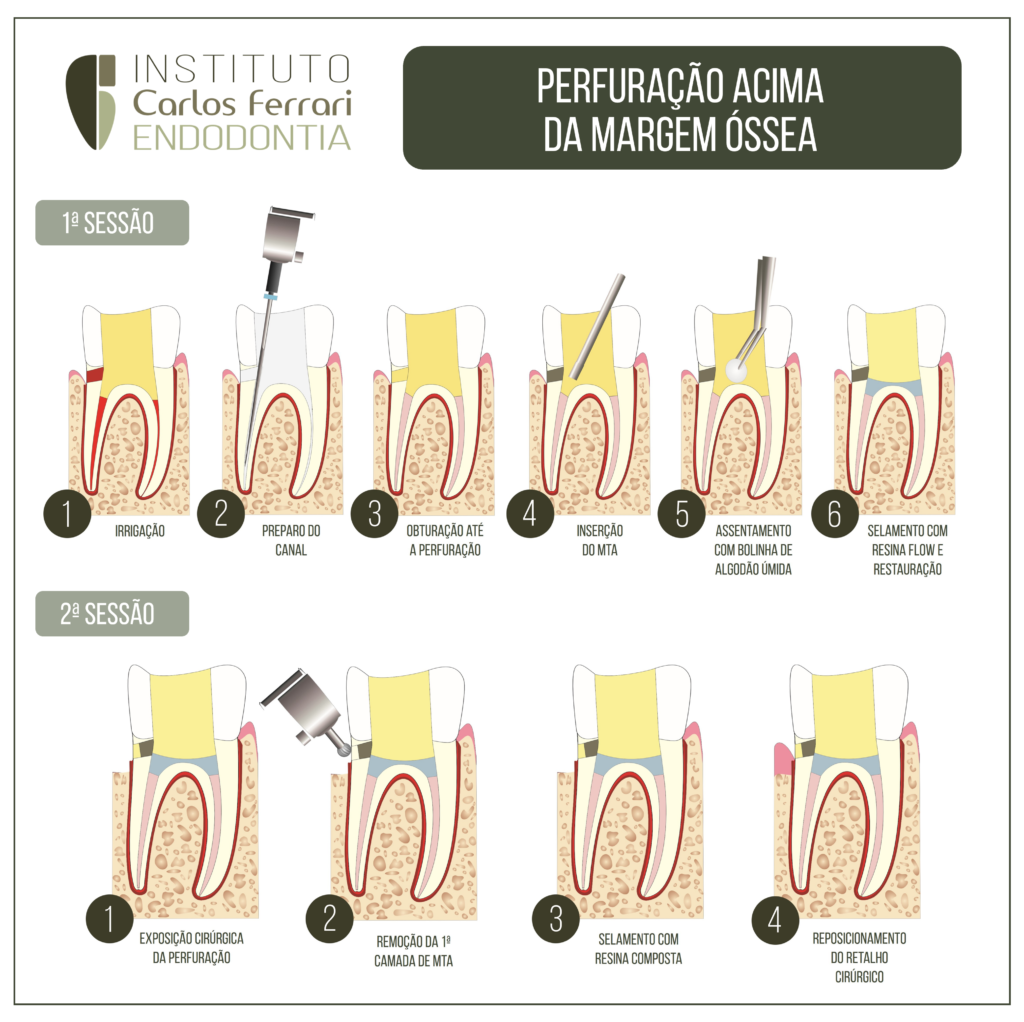
Perfuração lateral, acima da margem óssea . O que fazer?
Ocorreu uma perfuração durante a cirurgia de acesso e não há maiores danos ósseosacima da margem óssea?
A seguir um guia em caso de perfuração endodôntica imediata em perfurações laterais, tratados com materiais biocerâmicos e resina composta.
In: Fukunaga D, Barberini AF, Shimabuko DM, Morilhas C, Belardinelli B, Akabane CE. Utilização do agregado de trióxido mineral (MTA)no tratamento das perfurações radiculares: relato caso clínico. Revista de Odontologia da Universidade Cidade de São Paulo 2007 set-dez; 19(3):347-53
INTRODUÇÃO
Com os recursos de que a Odontologia moderna
dispõe, o tratamento endodôntico apresenta índice de
sucesso próximo a 95%, airma Grossman5 (1983); Ingle9
(1961). Porém, a possibilidade de insucesso existe
quando não se tem um conhecimento correto da anatomia dental e suas variações, das técnicas operatórias,
instrumentos e materiais utilizados, e não se realiza um
diagnóstico correto, ocasionando erros e acidentes durante sua realização.
A instalação de comunicações da cavidade pulpar
com os tecidos periodontais decorre de processos patológicos como lesões cariosas de grande extensão ou por
mecanismos iatrogênicos durante as manobras da terapia
endodôntica (incorreta direção de trepanação, desgaste
dentinário excessivo, uso inadvertido de instrumentos
rotatórios) ou também nos procedimentos restauradores
pós-endodontia (confecção de retentores intra-radicular). (Páttaro et al.15 2004)
Quanto a esses, o proissional consegue minimizá-los
utilizando técnicas acuradas, instrumentos mais seguros
e de fácil manuseio, conhecimento adquirido por meio
de leitura, pesquisa e prática clínica.
Podemos minimizar as conseqüências desses erros e
acidentes com o uso de materiais retroobturadores que
sejam reparador, selador, inerte, biocompatível, radiopaco, e tenham boa aderência à dentina.
Esses materiais podem ser amálgama, hidróxido de
cálcio, ionômero de vidro, resina composta e o MTA
(Agregado de Trióxido Mineral), entre outros. Por ser
um material relativamente novo no mercado, o MTA
tem sido alvo de grande número de pesquisas a respeito
de suas características, seu comportamento e indicações,
inclusive comparando-o aos materiais comumente utilizados atualmente. (Ruiz et al.17 2003).
O MTA foi desenvolvido por Mahmoud Torabinejad, professor e pesquisador da Universidade de Loma
Linda, Califórnia (EUA), tendo como suas indicações
clínicas o capeamento pulpar, pulpotomia (em dentes
com ápice radiculares não formados), polpas necrosadas
(na forma de “plug” apical), reparação de perfurações
radiculares, reabsorção interna, intracanal ou por meio
de intervenção cirúrgica, como material retro-obturador,
além de estimular a deposição de cemento radicular (Torabinejad e Chivian19,1999; Ruiz et al.17 2003). Este vem sendo estudado quanto ao seu potencial de selamento
entre o sistema radicular e a superfície externa do dente.
Realizando estudo em cães, Ford et al.4
(1995) observaram a utilização do MTA, comparado-o ao amálgama,
no tratamento de perfurações de furca. Os pesquisadores
efetuaram perfurações do assoalho das cavidades pulpares dos dentes, onde metade dos mesmos foram restauradas imediatamente com amálgama e MTA, e a outra
metade foi tratada, após uma exposição ao meio bucal
de seis semanas. Os resultados foram colhidos após quatro meses, mostrando que houve formação de cemento
sobre o MTA em 83,33%, sem presença bacteriana, ausência de proliferação epitelial, e inlamação moderada
em 16,66% dos casos, quando do tratamento imediato.
No grupo onde as perfurações icaram expostas ao meio
bucal, obteve-se formação de cemento sobre o MTA em
28,57%, sem presença bacteriana, proliferação epitelial
em 42,85% e graus de inlamação moderada em 28,57%
e severa em 28,57% dos casos. O MTA mostrou-se superior ao amálgama em todos os quesitos descritos.
Nakata et al.13 (1998) tiveram também como resultados, em seus estudos, a ausência de penetração bacteriana (Fusobacterium nucleatum) em todos os dentes
nos quais a perfuração foi selada com o MTA. O mesmo
ocorreu no estudo in vitro realizado por Torabinejad et
al.20,21 (1995) quanto ao poder de penetração bacteriana
do Staphylococcus epidermidis, no qual os resultados mostraram que o MTA não permitiu proliferação bacteriana,
durante o período do experimento (noventa dias)
Perfuração radicular com dano ósseo