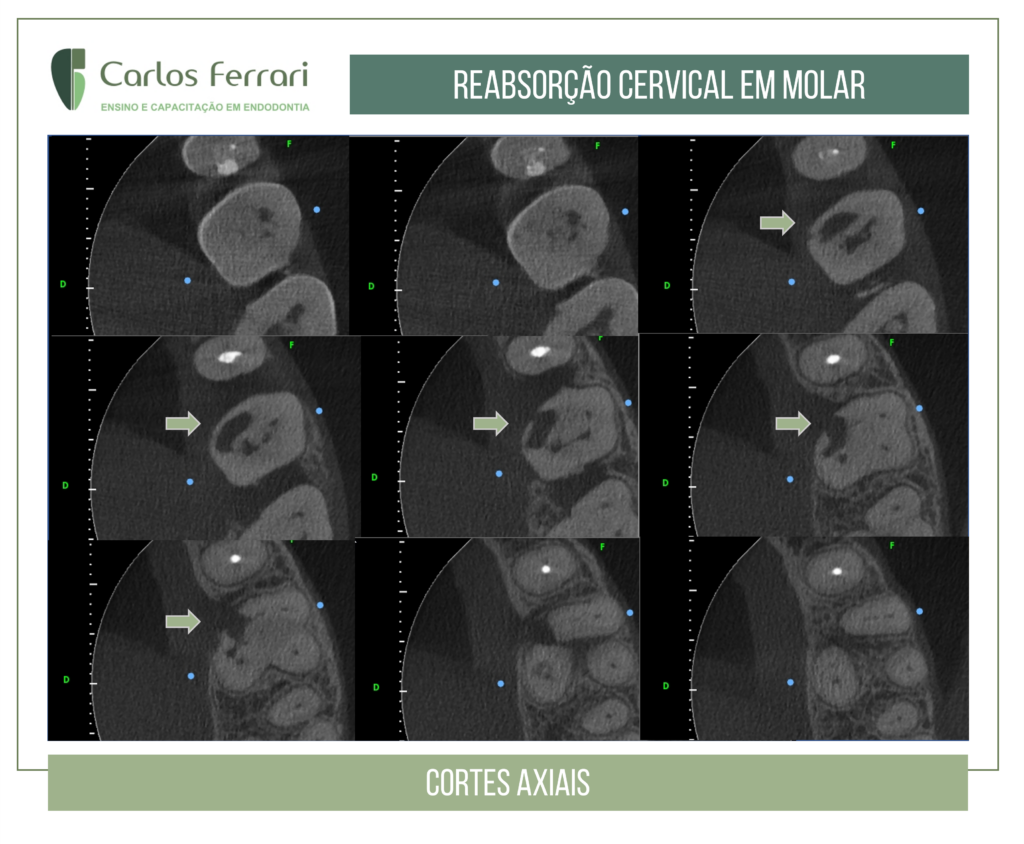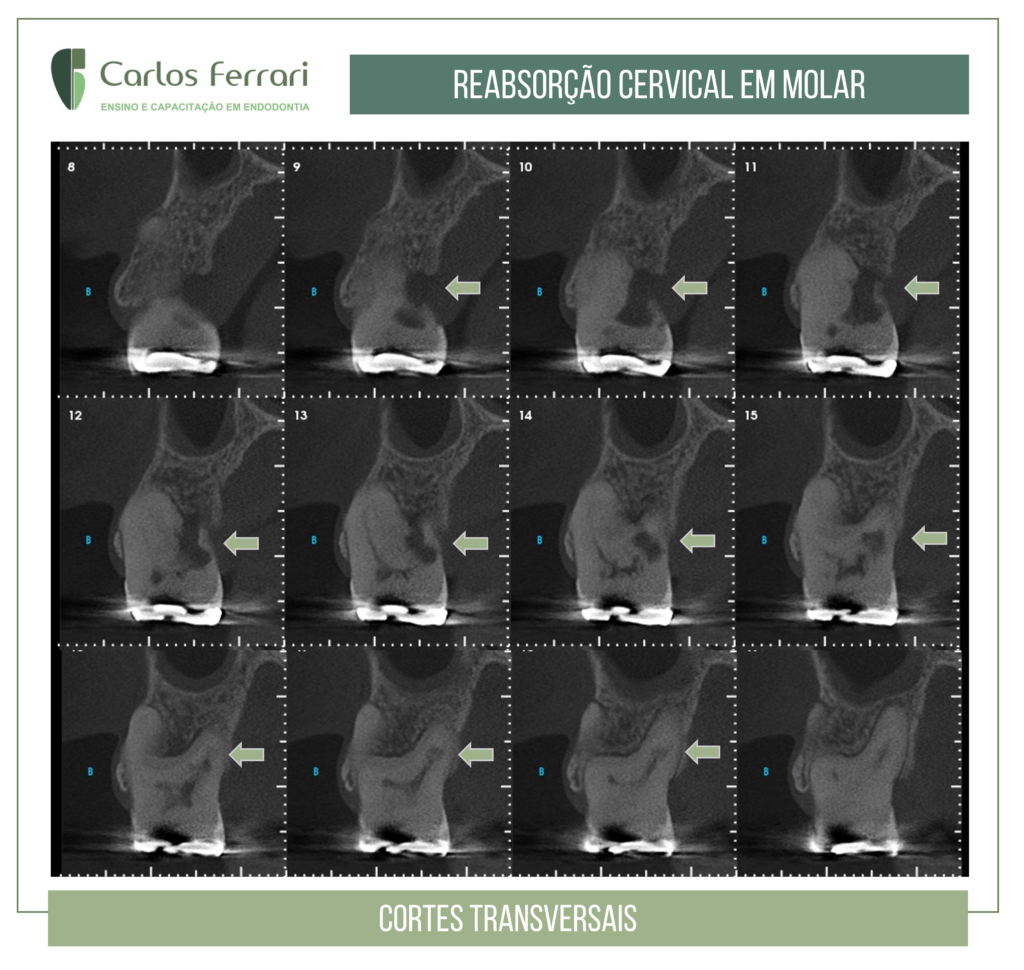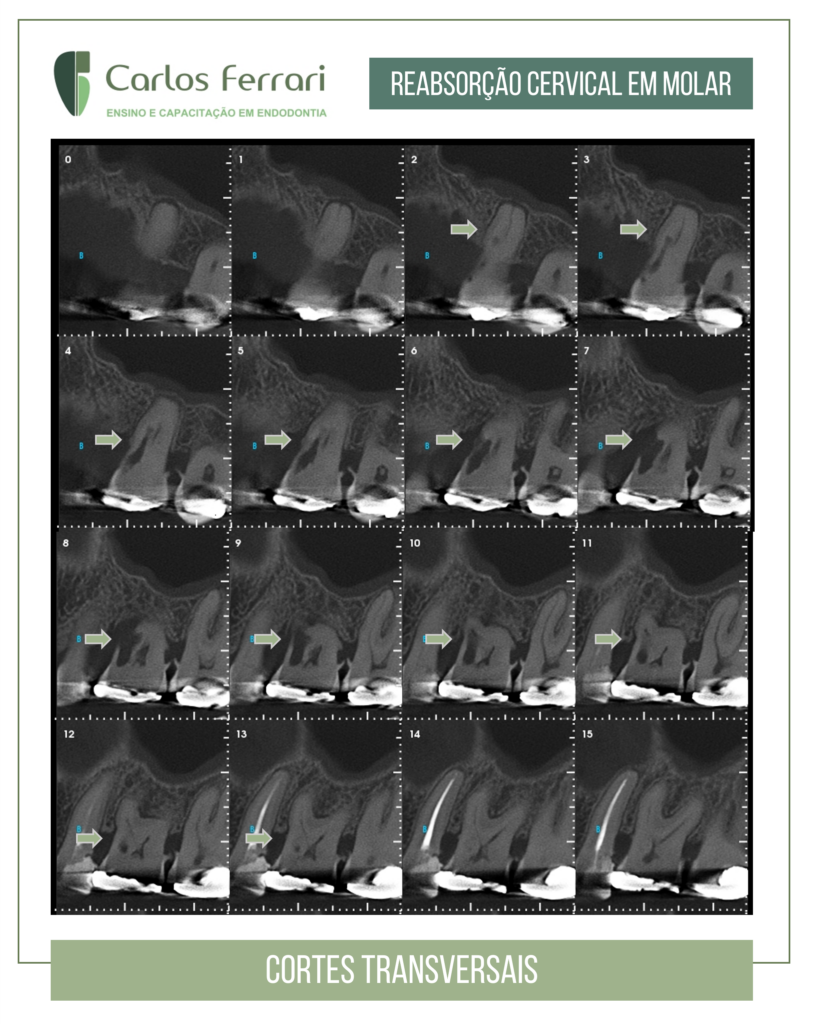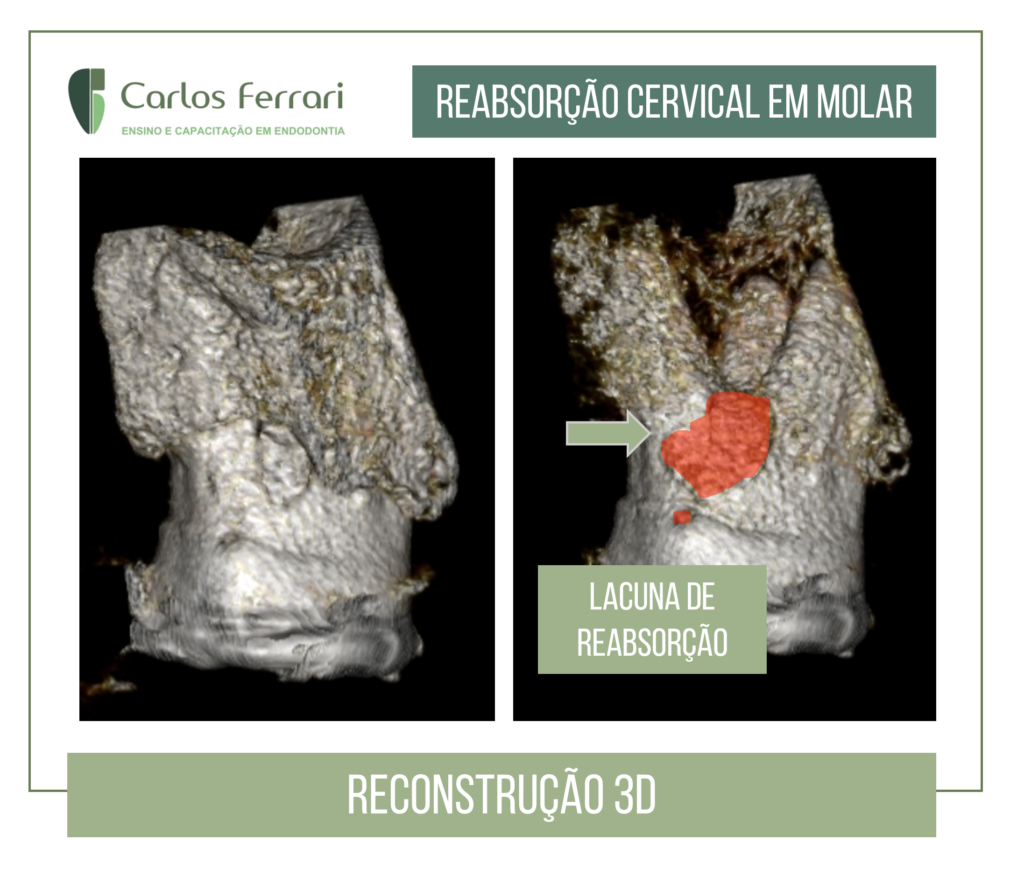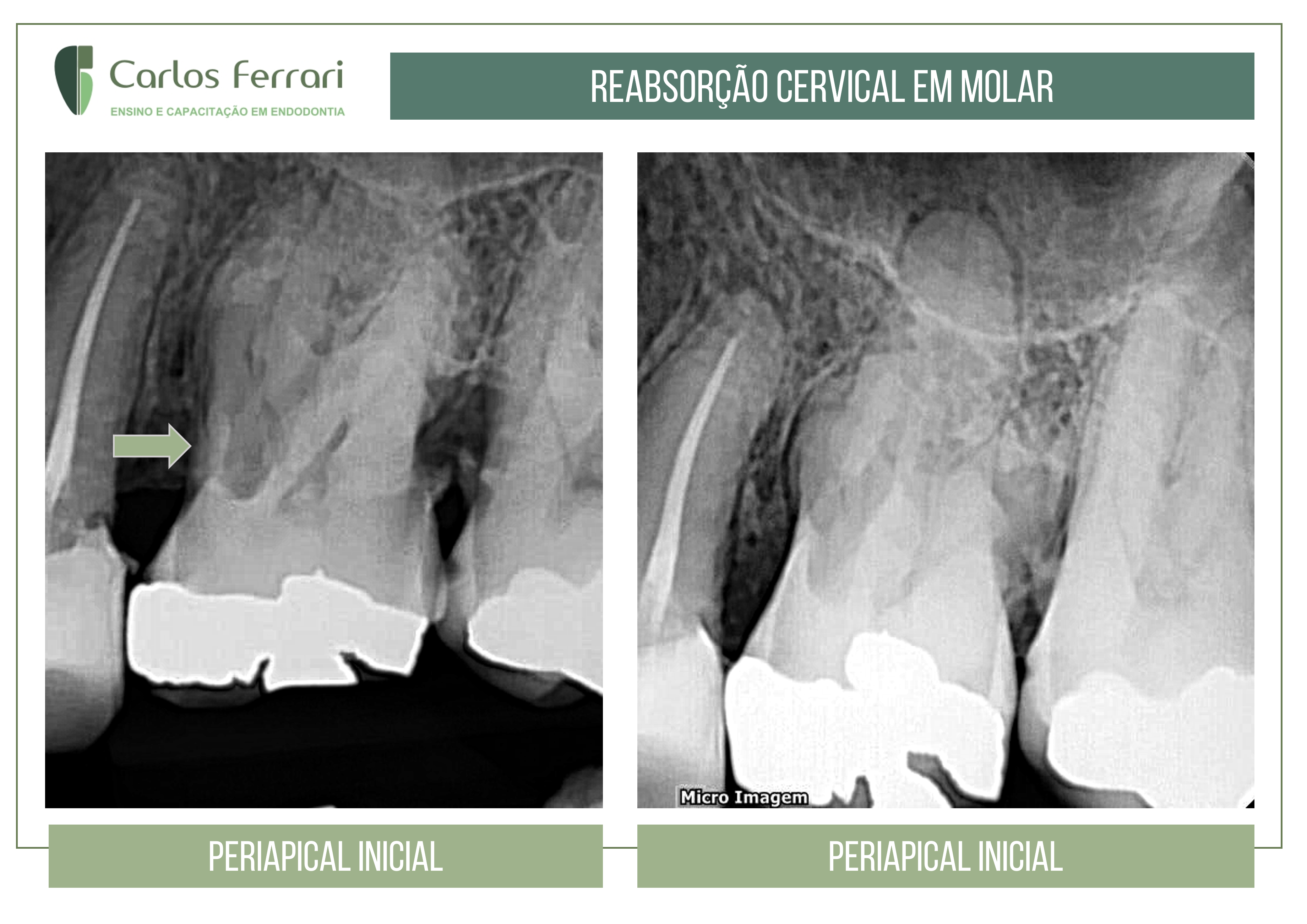
Inflammatory external cervical resorption. Patient sought care complaining of pain and swelling in the gingiva by palatine. Clinical examination revealed gingival edema and periodontal probing of 9 mm depth in the region. Palpation and percussion tests were negative and vitality was positive, with a more exacerbated response in relation to the other teeth, therefore, as a pulp diagnosis, asymptomatic irreversible pulp inflammation. Radiographic and tomographic examination revealed images compatible with external cervical resorption. The proposed treatment was endodontic and surgical with restoration of the resorbed area, by intentional reimplantation.
In: Machado, Ricardo. Endodontics: Biological and Technical Principles. Available at: GEN Group, GEN Group, 2022.
Invasive cervical external tooth resorption
They start in the cementoenamel junction after internal and/or external bleaching, trauma, surgical procedures, periodontal and/or orthodontic treatments. Its etiology is still not completely elucidated, but traumas are frequently associated with its occurrence. The most affected teeth are: upper canines and incisors, and lower molars (vital, necrotic or endodontically treated).
In vital teeth, initially there is no pulp involvement, because the pathological process originates in the periodontal ligament. Microorganisms and their by-products present in the gingival sulcus trigger an inflammatory reaction. Consequently, there is a release of chemical mediators responsible for resorption (cytokines and prostaglandins), which advance in the coronal and apical direction. Over time, pulp necrosis may occur, but normally resorption bypasses the pulp cavity without contacting it directly.
Heithersay (1999) proposed a classification for invasive cervical external tooth resorption considering its evolution.
Invasive cervical external tooth resorptions expand first in a coronal direction and then apically. In the early stages, the pulp remains healthy due to the presence of pre-dentin. In older resorptions (Class IV), there may be communication with the pulp cavity.63 Additional resorption pathways are also created reaching the apical periodontal ligament. The root structure is gradually compromised, assuming a beehive appearance.
Clinically, a pinkish spot can be observed in the cervical region near the gingival sulcus. In other cases, the tooth shows no perceptible changes. When there is vitality, the responses to thermal tests are within normal standards. In cases of necrosis or in teeth already treated endodontically, these responses are negative. During periodontal probing, significant bleeding is usually observed due to the presence of granulation tissue. The edges of the resorbed surfaces are sharp, thin, and brittle.
https://www.youtube.com/watch?v=xT6ugf6Z6r4
https://ferrariendodontia.com.br/reabsorcao-radicular-2/