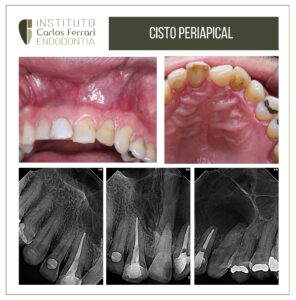
Dental trauma. Uncomplicated crown-root fracture.
A 15-year-old male patient came to the clinic complaining of a fractured tooth and reporting trauma while playing sports 15 days ago.
On clinical examination, crown retained by periodontal tissue in the palatal region, typical aspect of crown-root fracture. Clinical tests from canine to canine did not reveal any changes in the other teeth.
After anesthesia and removal of the fragment, exposure of the pulp chamber was observed. A crown augmentation and subsequent isolation and complete endodontic treatment were performed. The palatal portion was then removed, followed by conditioning of the crown fragment and tooth, and bonding was performed. The patient was instructed to return for revision and aesthetic finishing, and long-term preservation.
After 1 year, normal periodontal tissues and absence of signs and symptoms are observed.
Case conducted in the endodontics specialization clinic at HPG Brasília, together with Prof. Simone Sadalla.




Dental trauma. Complicated crown-root fracture. In: Machado, Ricardo. Endodontics: Biological and Technical Principles. Available at: GEN Group, GEN Group, 2022.
Introduction
Traumatic dentoalveolar injuries are a public health problem due to their high prevalence, especially in children and adolescents (3.9 to 58.6%). More than a billion people have suffered some type of dental trauma, and in Brazil, the last study showed that 20.5% of individuals aged 12 years had at least one traumatized incisor. Although the etiology of traumatic dentoalveolar injuries is known, prevention and control programs are not properly carried out, and therefore do not have the desired effect.
Immediate care (which precedes the dental surgeon's action) and subsequent professional conducts greatly influence the long-term prognosis. The aggressiveness of the trauma and/or the institution of inadequate approaches can cause or contribute to the occurrence of significant aesthetic-functional compromises, considering even the possibility of losing the teeth involved, which can harm the patient's biopsychic and emotional development.
Despite the remarkable technical and scientific development that has occurred in dentistry in recent decades, treatment alternatives for aesthetic resolution of dentoalveolar trauma are limited. As most patients are still undergoing craniofacial development, temporary interventions may be necessary before definitive rehabilitation is achieved.8 Moreover, multidisciplinary approaches and longitudinal follow-ups are essential to overcome difficulties and diagnose late sequelae, respectively.
In the following, philosophical, biological, and technical fundamentals for the treatment of traumatic dentoalveolar injuries will be presented.
Coronal fractures of enamel and dentin with pulpal exposure (complicated)
In complicated coronal fractures, there is loss of enamel and dentin, with exposure of the pulp tissue to the oral environment. Invariably, the pulp develops an inflammatory response triggered by bacterial agents and their by-products, and chemical mediators stimulated by the tissue laceration itself. This process results in the formation of a localized hyperplastic tissue with a depth of about 2 mm, provided that the apical vasculonervous bundle has not been ruptured.
In addition, the pulp exposure itself allows the drainage of the inflammatory edema, preventing increased pressure inside this tissue. However, long periods of exposure can lead to a more intense and deep inflammatory condition, with formation of microabscesses in the pulp. Thus, professional intervention should be performed as soon as possible, in order to preserve its vitality.
Dental trauma