


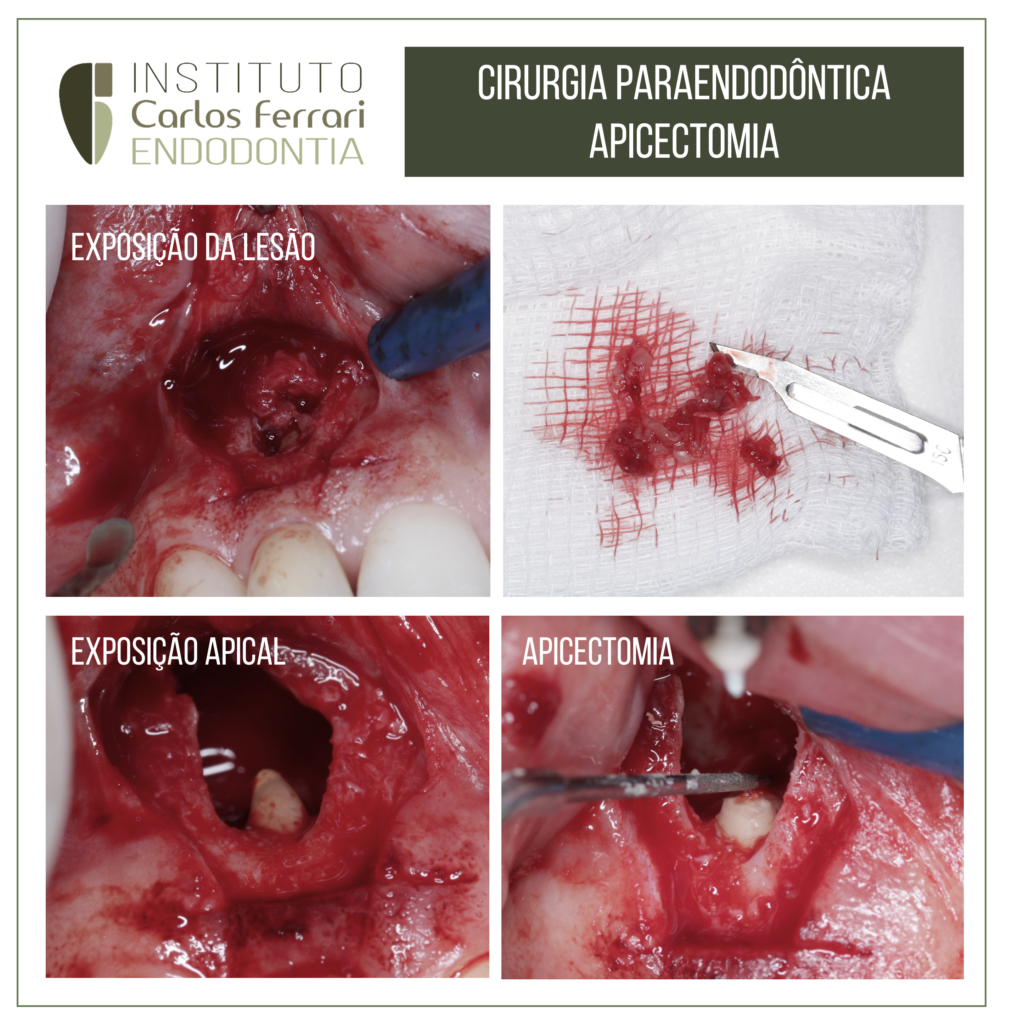
Apicectomia em cirurgia paraendodôntica.
Paciente passou por tratamento endodôntico do dente 12 com sucessivas trocas de medicação, sem remissão da fístula.
O canal foi então obturado para a realização de apicectomia com ponta de ultrassom.
Após 1 mês, a paciente teve melhora clínica e foi orientada para a proservação. Em 5 meses o quadro apresenta normalidade clínica e aparente reparo radiográfico.



Caso conduzido pelos alunos Joice Gandini e Igor Fajan da especialização em endodontia da APCD Bragança Paulista.
Cirurgia paraendodôntica e prótese fixa. In: Marchetti et al. Cirurgia paraendodôntica: relato de caso clínico. RSBO v. 5, n. 2, 2008
O paraendodonto compreende a região periapical, a zona perirradicular e regiões limítrofes, para as quais podem se estender as complicações endodônticas.
É sabido que o tratamento endodôntico deve proporcionar uma completa obliteração de todo o sistema de canais radiculares. O estabelecimento de um adequado selamento objetiva impedir que os microrganismos e/ou as endotoxinas atinjam os tecidos apicais e periapicais
Nas situações em que se constata fracasso naterapia endodôntica convencional após o dente estarrestaurado, com núcleo intracanal ou até mesmo como suporte de prótese fixa, está indicado o procedimento cirúrgico. Também em casos de lesões periapicais persistentes ou ainda com características císticas, canais radiculares calcificados com lesões periapicais onde é impossível o acesso via câmara pulpar, instrumentos fraturados, perfurações apicais e degraus, a forma de contornar e solucionar o problema é a indicação da cirurgia paraendodôntica.
Segundo Berbert et al. (apud Bernabé e Holland, a terminologia correta para esse procedimento é cirurgia paraendodôntica, pois abrange todos os tipos de intervenções cirúrgicas relacionadas ao endodonto. Durante muito tempo a cirurgia paraendodôntica foi domínio exclusivo do cirurgião bucomaxilofacial.
Recentemente passou a ser abordada pelo endodontista, que é o profissional mais indicado para realizá-la, pois é ele que conhece detalhadamente a anatomia da raiz e do canal e suas conseqüentes implicações em um processo periapical. A constante evolução das técnicas endodônticas faz com que os tratamentos de canais radiculares alcancem altos níveis de sucesso, mas esses procedimentos estão sujeitos a falhas e acidentes na sua execução.
Ante o fracasso do tratamento endodôntico podese optar pelo retratamento. Mas nos casos em que ele não é possível a cirurgia paraendodôntica é uma excelente alternativa para a resolução dos problemas não solucionados pelos tratamentos convencionais.
A cirurgia paraendodôntica constitui um conjunto de procedimentos com o objetivo de resolver complicações decorrentes de um tratamento de canal radicular ou seu insucesso. Ela é indicada quando não é possível ter acesso ao sistema de canais em dentes com lesão periapical, por causa de canais calcificados ou obstruídos por instrumentos fraturados, além de casos em que há material obturador extravasado, falha do tratamento convencional e impossibilidade de retratamento, perfurações apicais, dentes com núcleo ou portadores de prótese fixa.
As contra-indicações podem ser de ordem localou geral. As de ordem local ocorrem quando há possibilidade de tratar ou retratar o canal e quando há impossibilidade de acesso cirúrgico, suporte periodontal insuficiente, processos patológicos em fase aguda e risco de injúria a estruturas anatômicas. Algumas dessas contra-indicações podem ser minimizadas com a experiência do operador. Quanto às contra-indicações de ordem geral, citam-se precário estado geral de saúde do paciente e grau de comprometimento sistêmico.
As modalidades cirúrgicas mais usadas são a curetagem periapical, a apicectomia, a apicectomiacom obturação retrógrada, a apicectomia com instrumentação e obturação do canal radicular viaretrógrada e a obturação do canal radicular simultânea ao ato cirúrgico [10]. A curetagem periapical é um procedimento cirúrgico que tem a finalidade de remover tecido patológico em uma lesão no nível apical de um dente ou corpos estranhos na região periapical [5, 10]. Em algumas situações, em caso de necrose pulpar e lesão perirradicular, há formação de um biofilme periapical de difícil eliminação pelos procedimentos e medicamentos endodônticos convencionais. Essa camada é colonizada por bactérias que podem perpetuar a lesão perirradicular. Desse modo, devese realizar a curetagem periapical a fim de remover o biofilme microbiano. Para Leal et al, a curetagem deve ser sempre acompanhada de uma plastia apical, ou seja, alisamento cuidadoso do ápice radicular. Esse procedimento é necessário pois o cemento que recobre a porção apical da raiz se encontra reabsorvido.
A apicectomia é a remoção cirúrgica da porção apical de um dente. É indicada em inúmeras situações clínicas, tais como lesões periapicais persistentes ao tratamento convencional, perfurações instrumentos fraturados, remoção de deltas apicais, presença de reabsorção externa, entre outras
A apicectomia associada à obturação retrógrada consiste em remoção da porção apical de um dente, preparo de uma cavidade na porção final do remanescente radicular e obturação desse espaço com material adequado. Nos casos em que há necessidade de desinfecção e saneamento do canal radicular, realizam-se a sua retroinstrumentação e posterior retroobturação.
Já a obturação do canal simultânea ao ato cirúrgico consiste na curetagem periapical comapicectomia de um dente, seguida da obturaçãoconvencional do sistema de canais durante o atocirúrgico. Está indicada para resolver casos de extensas lesões periapicais crônicas em que o canal está bem instrumentado e já foram feitas inúmeras trocas de hidróxido de cálcio, no entanto há presença de exsudato inflamatório impedindo a conclusão do caso .
Diversos autores têm relatado casos de cirurgia paraendodôntica na literatura, mostrando a diversidadede situações clínicas e técnicas empregadas. Mariano e Messora realizaram apicectomia nos dentes com extensa perda óssea periapical e, como havia ausência de suporte ósseo para apoio do retalho, utilizaram membrana de colágeno para guiar a regeneração tecidual. Na proservação radiográfica do caso por quatro anos, observaram redução completa da área radiolúcida com bom reparo ósseo.
Rosa et al. descreveram um caso de apicectomia associada à obturação retrógrada com MTA em um dente portador de prótese fixa com lesão periapical, obtendo neoformação de tecido ósseo num período de sete meses.
A escolha do material retroobturador é de fundamental importância para o sucesso da cirurgia paraendodôntica. As características ideais do material retroobturador devem ser: não-tóxico, nãomutagênico, biocompatível e insolúvel. Além disso, deve possuir adesão à estrutura dentária e manter sua capacidade seladora por longo período, além de ser de fácil manipulação, radiopaco, ter estabilidade dimensional e não ser afetado na presença de umidade.
Cirurgia paraendodôntica e prótese fixa.


