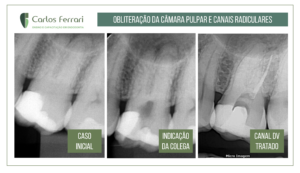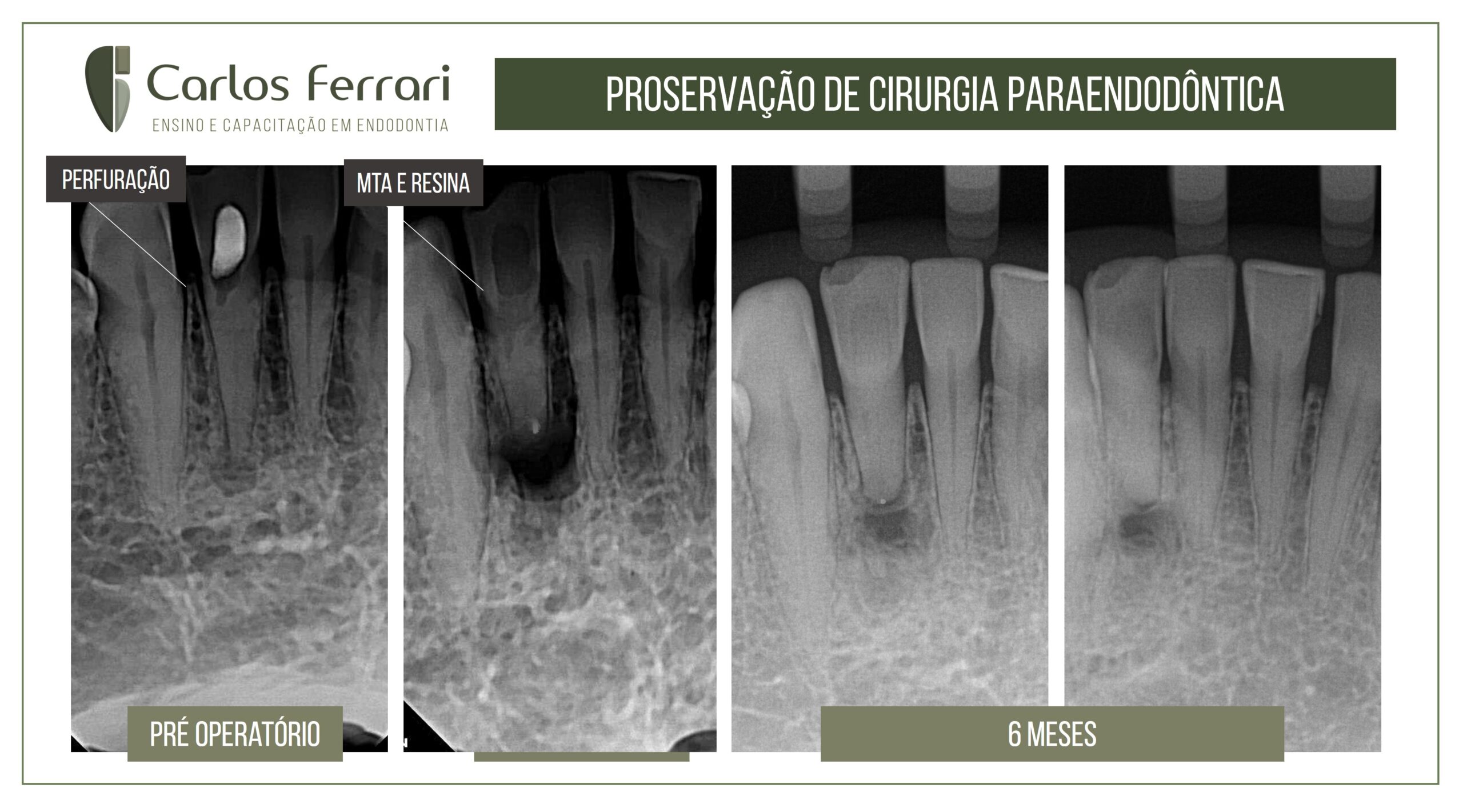
Cirurgia paraendodôntica, proservação de caso. Há casos em que precisamos analisar as alternativas de tratamento levando-se em conta vários fatores.
Esse paciente foi encaminhado por um colega após tentativa de acessar o canal radicular calcificado do dente 42. A paciente tinha quadro de abscesso periapical agudo e imagem radiográfica radiolúcida periapical. Após o exame clínico julgamos temerária a utilização de guia de acesso, pelo tamanho do dente, muito pequeno e delicado e por já haver desgastes na coroa.
O tratamento escolhido foi então o selamento o espeço coronário com MTA e a cirurgia paraendodôntica e retropreparo e obturação também com MTA.
O pós-operatório, além de ausência clínica de sinais e sintomas e tecidos normais, mostra radiograficamente reparação tecidual em andamento. A paciente foi orientada para nova proservação dentro de 1 ano.
https://ferrariendodontia.com.br/cirurgia-canal-calcificado/
A terapia endodôntica apresenta diversos desafios durante a sua realização, sendo que o principal deles é a complexidade anatômica. A total eliminação dos microrganismos responsáveis pelo desenvolvimento ou pela manutenção de uma lesão periapical é infactível, justamente em razão de eles estarem presentes dentro de um emaranhado sistema de canais radiculares. O tratamento endodôntico visa, portanto, diminuir ao máximo esse contingente microbiano a níveis favoráveis ao reparo.
Bactérias se organizam em biofilmes para potencializar sua resistência antimicrobiana e patogenicidade. A eliminação dessas comunidades ocorre, sobretudo, por meio da ação mecânica dos instrumentos endodônticos. Todavia, estes não são capazes de tocar todas as paredes do canal, sendo, portanto, essencial para a eliminação do biofilme intrarradicular, o uso de substâncias químicas auxiliares capazes de dissolver matéria orgânica, dentre as quais se destaca o hipoclorito de sódio. Outras alternativas para intensificar o controle da infecção endodôntica são o uso de diferentes substâncias como medicação intracanal, a ativação das soluções irrigantes e a terapia fotodinâmica. Ainda assim, a completa erradicação da infecção endodôntica ainda não pôde ser alcançada.
Diante de um insucesso endodôntico primário, três possibilidades de tratamento são normalmente consideradas (em ordem de preferência): o retratamento endodôntico, a cirurgia paraendodôntica e a exodontia, seguida pela instalação de um implante dentário. A cirurgia paraendodôntica representa uma alternativa para casos de insucesso após o retratamento ou para a resolução de erros e acidentes ocorridos anteriormente.
Em várias situações, pacientes e profissionais têm dúvidas sobre a melhor alternativa a ser instituída ao compararem a cirurgia paraendodôntica com a extração seguida pela colocação de um implante. Nesses casos, deve-se avaliar bem o custo-benefício de ambos os procedimentos. Determinados fatores podem contribuir para a tomada dessa decisão, dentre os quais destacam-se a idade e as condições sistêmica e financeira do paciente, a localização e a proximidade do dente com estruturas anatômicas nobres, a quantidade de osso remanescente, o comprimento radicular e a extensão da lesão periapical (quando presente).
Revisões sistemáticas e metanálises apontam para um aumento dos índices de sucesso das cirurgias paraendodônticas quando realizadas sob “à luz da microscopia operatória” e utilizando materiais retro-obturadores, principalmente o agregado trióxido mineral (MTA). Assim, o procedimento é capaz de prolongar a manutenção dos dentes na cavidade oral, postergando a instalação de implantes. Iqbal e Kim, em 2008,17 observaram que, sempre que possível, os pacientes preferiam manter seus dentes naturais a partir da instituição de diferentes alternativas (tratamento, retratamento e cirurgia paraendodôntica) em vez de substituí-los por implantes.
In: Machado R. Endodontia. Princípios Biológicos e técnicos. Capítulo: Cirurgia Paraendodôntica. Ed. Gen, 2022.