


Reabsorção externa.
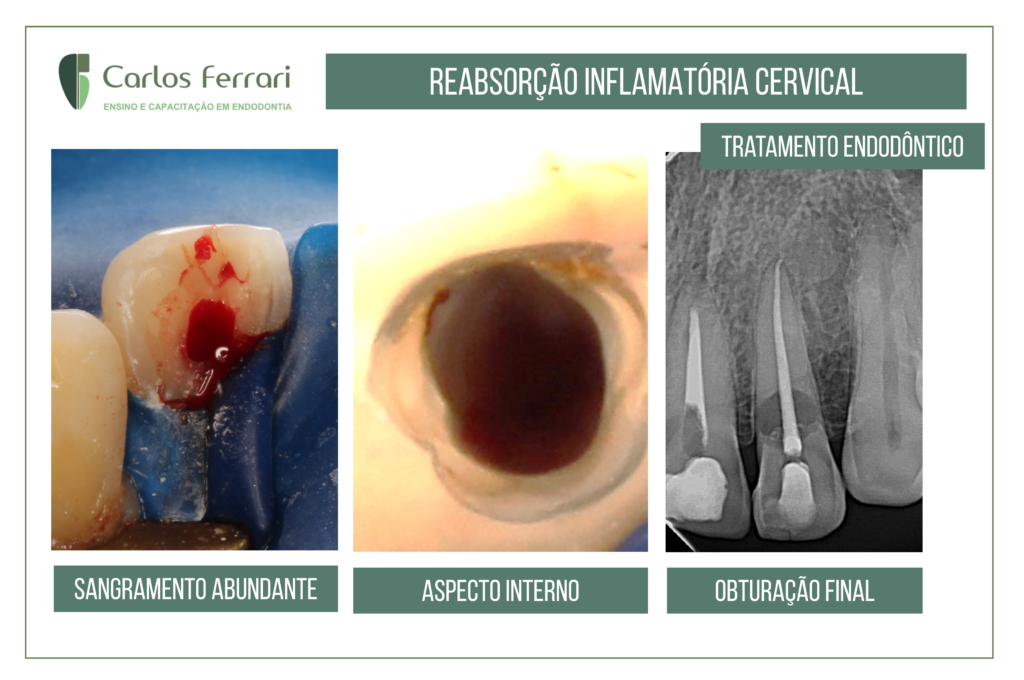
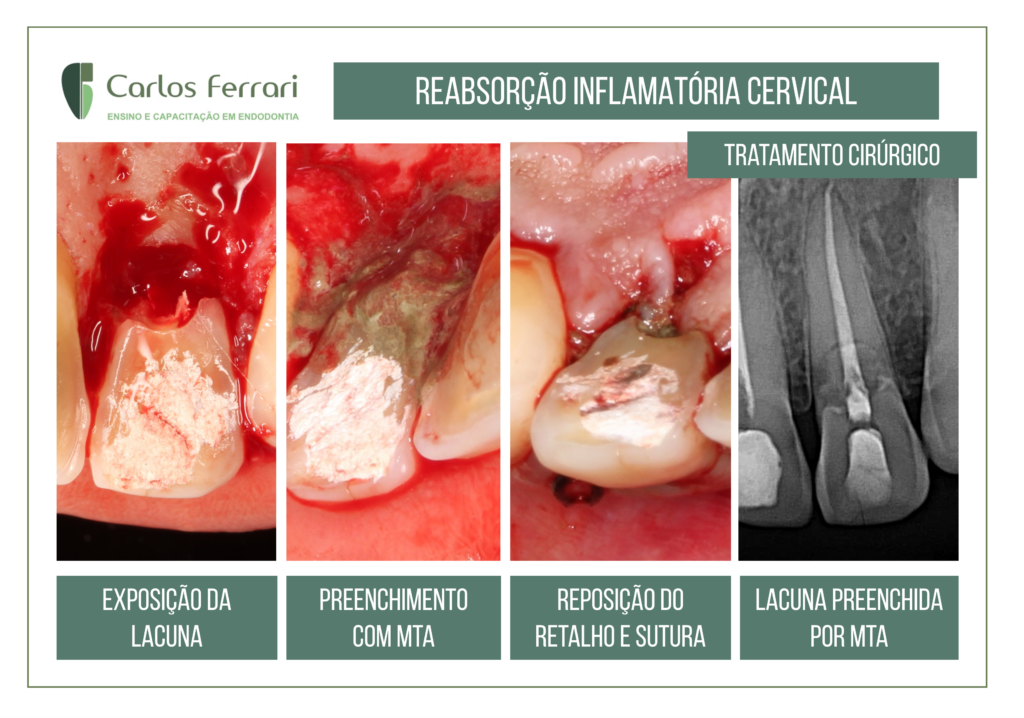
Paciente procurou a clínica queixando-se de dor ao quente e gelado, com declínio lento. No exame clínico, constatou-se lacuna de reabsorção na superfície cervical palatina. O exame radiográfico revelou imagem radiolúcida característica de reabsorção cervical inflamatória. O tratamento realizado foi endodôntico, cirurgia periodontal, fechamento da cavidade de reabsorção com MTA e resina composta na cervical.
O acompanhamento de 2 meses revela aspecto saudável dos tecidos adjacentes à lesão.
Caso realizado pelos alunos Sinuhe Saad e Bruno Cavalcante da turma II da especialização em Endodontia da HPG Brasília.
In: Barnabé et. al. Rev Odontol Bras Central 2011;20(55)
Reabsorção cervical externa é uma forma de reabsorção dentária externa relativamente rara e de natureza invasiva, geralmente sua causa está associada a trauma dentário, tratamento ortodôntico ou clareamento interno. Por não apresentar sintomatologia dolorosa, muitas vezes é diagnosticada por examesradiográficos de rotina, dificultando seu diagnóstico no estágio
inicial.
Reabsorção cervical externa (RCE) é um termo clínico utilizado para descrever uma forma de reabsorção dentária externa
relativamente rara e de natureza invasiva que pode ocorrer em qualquer dente na dentição permanente. Caracterizada pela
sua localização cervical, este processo leva à reabsorção progressiva e geralmente a perda destrutiva da estrutura dental².
Embora se saiba que uma das funções do cemento seja proteger a dentina radicular de ser reabsorvida, qualquer dano causado a esse tecido pode resultar na exposição de dentina radicular aos osteoclastos e, portando, iniciar o processo de reabsorção, Atualmente, pouco se sabe sobre a etiologia da RCE. Alguns fatores predisponentes têm sido sugeridos como desencadeadores do processo de reabsorção. Os mais significativos são o trauma dentário, tratamento ortodôntico e clareamento interno.
A condição é geralmente indolor, exceto quando acompanhada de infecção pulpar ou periodontal, portanto é muitas vezes
diagnosticada por exames radiográficos de rotina.
Quando a lesão torna-se visível, as características clínicas podem variar de
um pequeno defeito na margem gengival a um aspecto róseo na coroa do dente, sendo evidenciada devido a reabsorção dentinária e ao tecido altamente vascular que se torna visível através do fino esmalte remanescente.
Heithersay (1999) classificou as lesões de acordo com a sua extensão: Classe I, uma pequena lesão com reabsorção perto da área cervical com penetração em dentina superficial; Classe II, lesão com extensão em direção à câmara pulpar coronária,
mas mostra pouca ou nenhuma invasão da dentina radicular; Classe III, profunda reabsorção que envolve a dentina coronal, mas também se estende para o terço cervical da raiz e Classe IV, processo de reabsorção grande que se estende além do terço cervical do canal radicular.

https://ferrariendodontia.com.br/reimplante-intencional-reabsorcao-radicular/


