

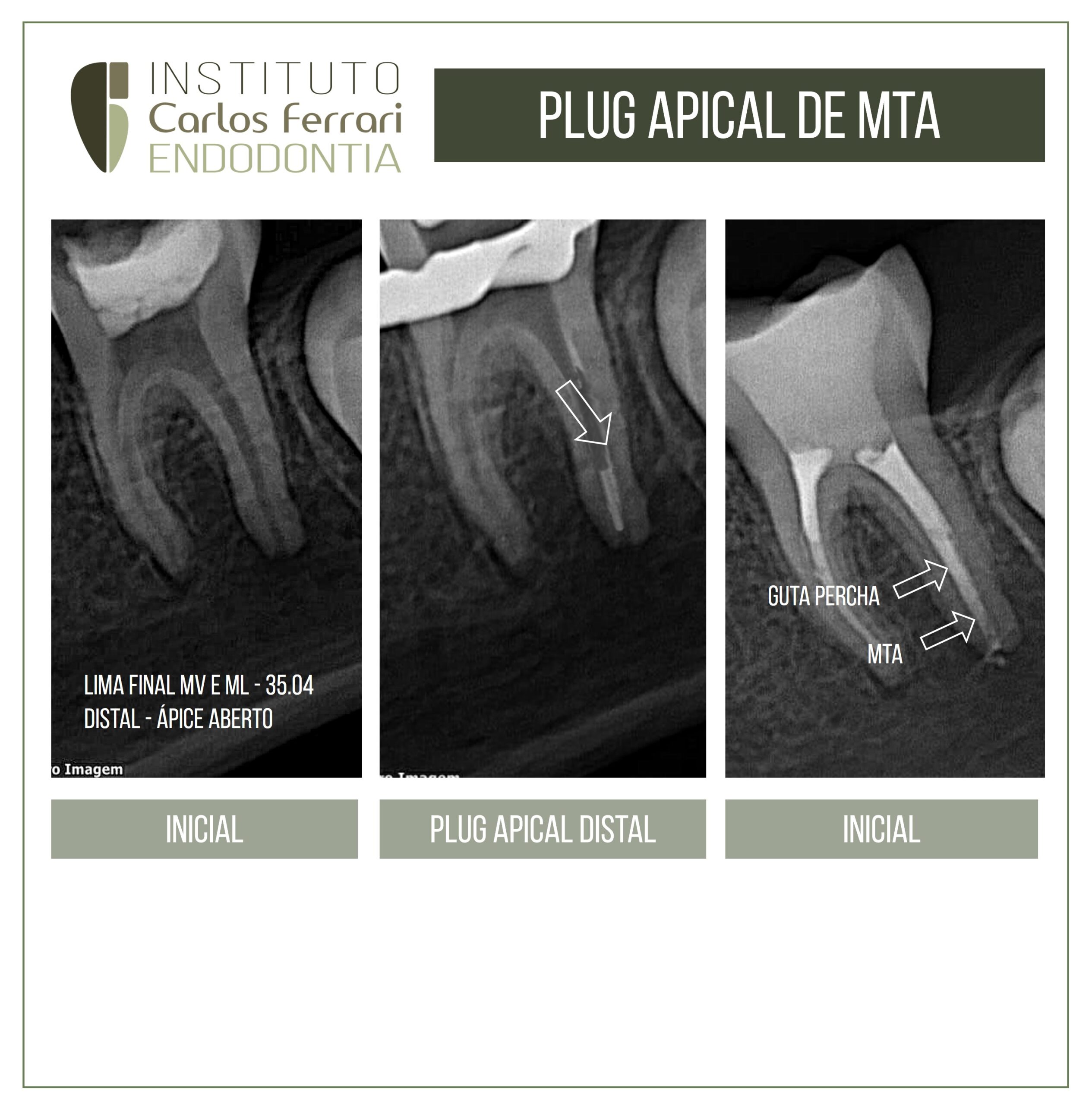
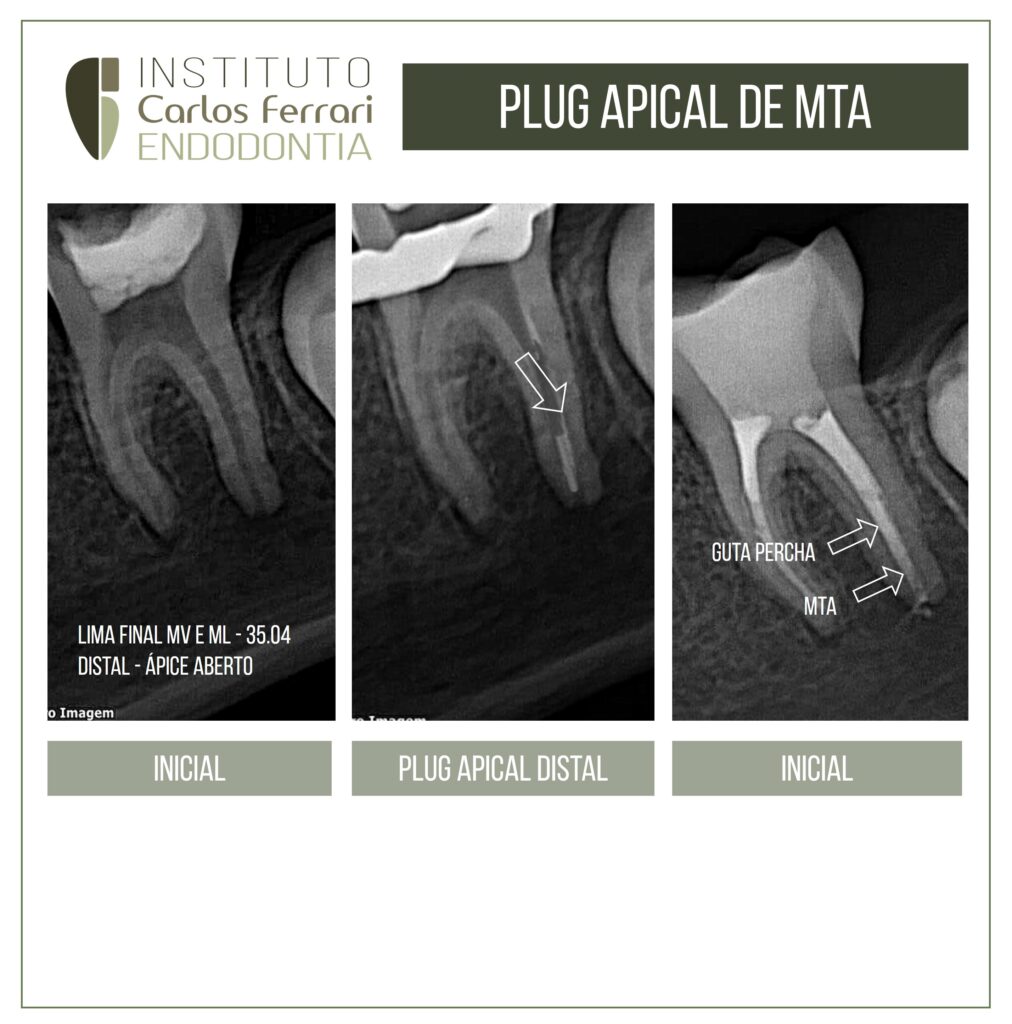
Plug apical de MTA em dente com rizogênese incompleta.
Paciente 11 anos, encaminhado para tratamento após procedimento de urgência endodôntica.
No exame radiográfico, imagem de provável formação radicular incompleta na raiz distal.
Durante o tratamento, conseguiu-se o travamento de cone 35.04 nos canais mesiais, porém no canal distal, houve grande dificuldade para ajuste de um cone de guta percha.
Procedeu-se então a colocação de um plug de MTA Repair, com cerca de 4mm, colocado com um porta MTA e assentado com uma lima envolta em algodão. Acima deste, foi realizada obturação convencional com guta percha e cimento Bio C Sealer.
Caso realizado pela aluna Luciane Felício, de especialização em Endodontia da Chibebe Cursos, Taubaté.
In: Castro et al. Avaliação da utilização de MTA como plug apical em dentes com ápices abertos. Rev. bras. odontol., Rio de Janeiro, v. 68, n. 1, p. 59-63, jan./jun. 2011
Introdução
Técnicas endodônticas convencionais de preenchimento dependem da presença de uma constrição em nível apical do canal, portanto, a ausência da constrição apical por causa do desenvolvimento radicular incompleto apresenta um desafio de gestão. O preenchimento da raiz de um canal amplo com um forame apical aberto acarreta o risco de extrusão de material obturador, o que pode comprometer o resultado a longo prazo do tratamento. Para evitar a extrusão, a compactação pode ser minimizada, resultando em inadequada adaptação e vedação. A maioria dos fracassos endodônticos ocorre como resultado de vazamento de substâncias irritantes presentes nos canais radiculares para os tecidos perirradiculares, portanto, um material de reparação deve proporcionar uma satisfatória vedação para o canal de raiz com ápice aberto.
Um dos critérios mais importantes para um material ideal endodôntico é a sua capacidade de selamento e adaptação marginal. Das opções disponíveis atualmente para o tratamento de canais radiculares com um vértice aberto, o uso de curativo de hidróxido de cálcio para induzir uma barreira de tecido duro apical (apicificação) caracteriza-se como um tratamento tradicional. Esta técnica foi introduzida pela primeira vez por KAISER (18) e, posteriormente, popularizada por FRANK (12). Apesar de apresentar um alto índice de sucesso, existem várias desvantagens desta técnica. Este procedimento normalmente requer várias visitas ao dentista em um período de 5-20 meses e durante este período, o dente é restaurado apenas temporariamente, tornando-o mais susceptível à infiltração coronária. Há também um maior custo do tratamento e risco de que o paciente possa deixar de seguir com as visitas necessárias. Além disso, a exposição prolongada ao hidróxido de cálcio pode afetar adversamente as propriedades mecânicas da dentina radicular tornando-o mais suscetível à fratura. A fragilidade e a porosidade da barreira apical calcificada formada nessa técnica resultam na possível extrusão apical da guta-percha durante o tratamento.
A indução de barreiras apicais artificiais com diferentes materiais tem sido sugerida como uma alternativa ao uso tradicional de hidróxido de cálcio (7). Uma dessas alternativas para induzir a apicificação é selar o forame apical aberto com um plug apical de Agregado Trióxido Mineral (MTA) (28). A popularidade do MTA como uma barreira artificial apical pode ser atribuída a vários fatores. Este procedimento pode ser concluído em uma ou duas sessões de tratamento, criando um stop apical na extremidade aberta do canal, tornando possível restaurar o dente dentro de um curto espaço de tempo com uma restauração adaptada à coroa, tornando-a significativamente mais forte do que as coroas não restauradas, reduzindo a possibilidade de fratura coronária. Ao contrário do uso prolongado de hidróxido de cálcio nas raízes imaturas, o preenchimento prolongado de raízes com MTA não reduz a suaresistência à fratura. A apicificação induzida com MTA também pode resultar em uma melhorconsistência da barreira apical de tecido duro e satisfatórias propriedades de selamento. Este processo só terá êxito se o espaço do canal radicular for fechado, evitando a entrada de novas bactérias, sepultando micro-organismos remanescentes e impedindo a sua sobrevivência, obstruindo o fornecimento de nutrientes. O MTA também proporciona uma vedação eficaz na dentina e cemento e promove o reparo biológico e regeneração do ligamento periodontal.
O MTA não só cumpre o requisito ideal de ser bacteriostático, podendo apresentar também propriedades bactericidas. A liberação de íons hidroxila, um pH elevado sustentado por períodos prolongados e a formação de uma camada mineralizada intersticial podem proporcionar um ambientedesafiador para a sobrevivência de bactérias. Essas propriedades antibacterianas podem ser um potente inibidor docrescimento bacteriano contra espécies como o Estreptoccocus faecalis, um micro-organismo prevalente em falhasde canal radicular. Além disso, a Candida Albicans, comumente presente na doença endodôntica refratária é suscetível à atividade antifúngica de MTA.
perfuração de furca em molar


